




 ometimes it is helpful to dispose of the high-intensity signal of fat or fluids. There are numerous suppression techniques. Two of them are inversion-recovery methods; additional techniques are discussed in Chapter 11.
ometimes it is helpful to dispose of the high-intensity signal of fat or fluids. There are numerous suppression techniques. Two of them are inversion-recovery methods; additional techniques are discussed in Chapter 11.
Images with long TI have little contrast between neighboring tissues, except the one created by differences in proton density, whereas images with short TI can show high contrast.
This feature is exploited in a special inversion-recovery pulse sequence, the STIR sequence.
 STIR (Short TI Inversion Recovery) sequences are often used when looking for high signal intensity lesions such as contrast-enhancing tumors close to or within fatty tissue because this IR sequence facilitates the suppression of the signal stemming from fat.
STIR (Short TI Inversion Recovery) sequences are often used when looking for high signal intensity lesions such as contrast-enhancing tumors close to or within fatty tissue because this IR sequence facilitates the suppression of the signal stemming from fat.
The fat signal reaches zero signal intensity at TR > 3000 ms, TI ~ 200 ms, and TE 20 ms (at 1.5 T); TI is lower at lower field strength (Figure 10-10).
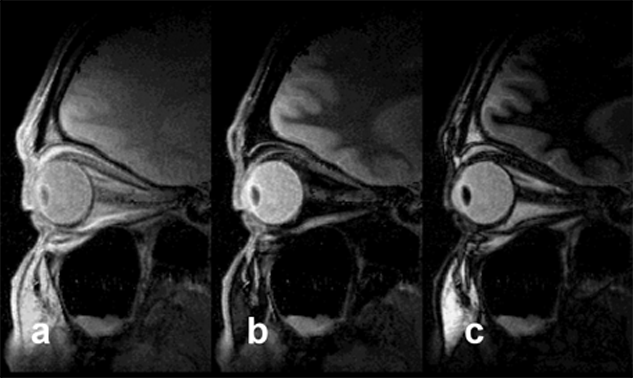
Figure 10-10:
STIR. In all images, TR = 4000 ms, TE = 10 ms; (a) TI = 50 ms, (b) TI = 240 ms, (c) TI = 450 ms. The fatty tissue close to the optic nerve disappears with a TI of approximately 240 ms. Signal suppression is based on T1 relaxation times and not tissue specific. STIR should be used before injecting contrast agents.
Signal suppression by STIR pulse sequences is based on T1 relaxation times; therefore it is not tissue specific. This is the reason why STIR sequences should be used before the administration of contrast agents that facilitate T1 shortening [⇒ Krinsky 1996].
To ensure effective characterization of tissue, selective fat suppression techniques are offered by different companies; they should be used whenever a substrate is isointense with respect to fat on multiple pulse sequences and the substrate is suppressed on STIR imaging. Details of these suppression techniques are discussed in Chapter 11.
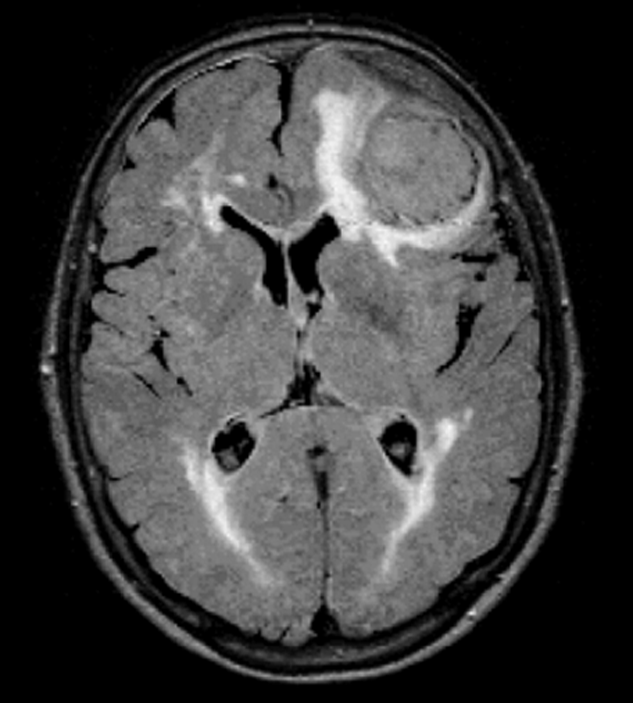
Figure 10-11:
FLAIR. TR = 8000 ms, TE = 120 ms, TI = 2000 ms. The brain lesions caused by the pressure of huge meningioma are well seen on the FLAIR image.
FLAIR (Fluid Attenuated Inversion Recovery) eliminates the signal from cerebrospinal fluid by using very long inversion times (2000–2500 ms). It is especially useful in brain lesions with low contrast (Figure 10-11).
CSF reaches the null point of no signal at an inversion time of ~2000 ms (TR > 8000 ms; TE > 100 ms), depending on field strength [⇒ De Coene 1992].
Both techniques can be combined with RSE sequences; they then become Fast STIR and Fast FLAIR.



|

|
|---|